 Main Facts:
Main Facts:
- The World Health Organization defines FGM as “procedures that intentionally alter or cause injury to the female genital organs for non-medical reasons” (1)
- Violation of human rights
- No health advantages for women
- Usually performed between infancy and age 15 (1)
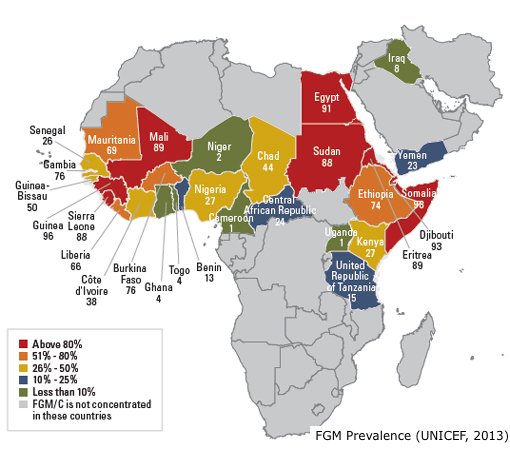
- Over 200 million girls and women have been subjected to FGM in 30 countries, mainly in Africa, the Middle East, and Asia, yet there are cases in North America, South America, Europe and Australia (1)
- Known as “vacation cutting,” families in the United States seeking the procedure may send their daughter to a country where the practice is accepted to undergo FGM (2)
Types of FGM:
4 main types (3):
- Type 1: partial or total removal of the clitoral glans (the external part of the clitoris, which is extremely sensitive), and/or the prepuce (the fold of skin surrounding the clitoris).
- Type 2: partial or total removal of the clitoral glans and the labia minora (the inner folds of vulva), with or without removal of the labia majora (the outer folds of vulva).
- Type 3: narrowing of the vaginal opening through the creation of a covering seal. Seal is formed by cutting and sewing over the outer labia, with or without removal of the clitoris or inner labia. This is known as infibulation.
- Deinfibulation refers to the practice of cutting open the sealed vaginal opening of a woman who has been infibulated to allow intercourse and childbirth.
- Type 4: all other harmful procedures to the female genitalia for non-medical purposes, e.g. pricking, piercing, incising, scraping and cauterizing the genital area.
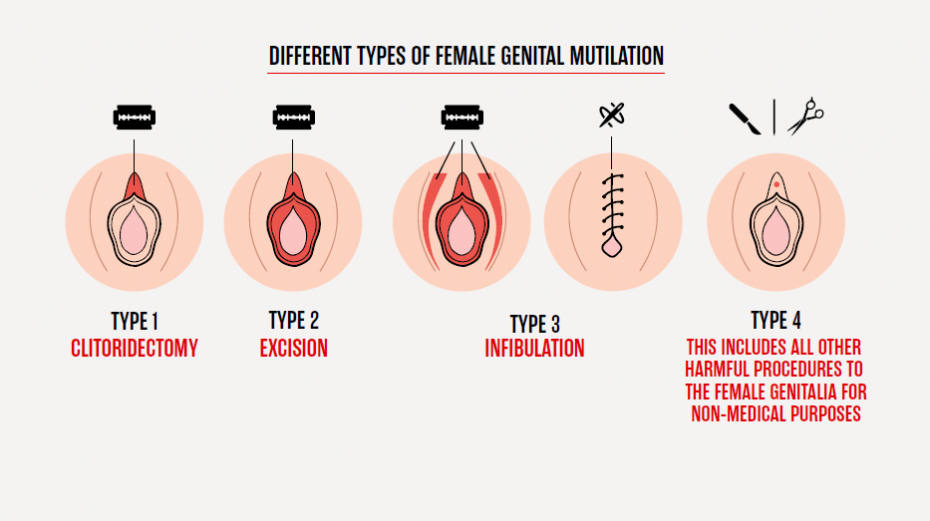
Types of FGM (www.rage.com)
Procedure Setting:
There is no formal standardized procedure (1):
- No such thing as “safe” FGM
- Mostly carried out by traditional circumcisers (non-medically trained), who often play other central roles in communities
- Unsterilized tools often used (bits of broken glass, needles, razors, knives)
- Girls are usually not provided with anesthesia and anesthetic
“Medicalization” of FGM:
- Medicalization of FGM is when FGM is performed by a health-care provider, such as a community health worker, midwife, nurse or doctor
- THIS IS NOT A MEDICAL PROCEDURE!
- FGM can never be “safe” even when performed in a sterile environment and by a health-care professional (4)
- “Medicalization” gives a false impression of security
- When performed in a clinical setting, FGM violates medical ethics and gives impression that it is without health consequences, which can undermine efforts towards abandonment (5)
Read more on the Meaning of FGM “Medicalization”
Health Risks:
Immediate risk (1):
- Severe pain
- Excessive bleeding
- Genital tissue swelling
- Fever
- Infections (e.g., tetanus)
- Urinary problems
- Wound healing problems
- Injury to surrounding genital tissue
- Shock
- Death
Long-term risk (1):
- Urinary problems (painful urination, urinary tract infections)
- Vaginal problems (discharge, itching, bacterial vaginosis)
- Menstrual problems (painful menstruations, difficulty in passing menstrual blood)
- Scar tissue and keloid
- Sexual problems (pain during intercourse, decreased satisfaction)
- Increased risk of childbirth complications and newborn deaths
- Psychological problems (depression, anxiety, post-traumatic stress disorder, etc.)
Violation of Human Rights:
- An extreme form of violence and discrimination against girls and women
- Violates principles of equality on the basis of sex
- Violates right to life (when the procedure results in death)
- Violates right to freedom from torture or cruel, degrading treatment or punishment
- Violates rights of the child
 Eliminating FGM:
Eliminating FGM:
- Many actions have been made to counteract FGM by working with communities, creating intervention plans, and passing laws (click here to learn more).
- While the prevalence of FGM has decreased in some countries, prevalence in many communities still remains high. There is still a pressing need to expand elimination efforts.
- Thus, being culturally understanding is of utmost importance. Creating a comfortable dialogue encourages FGM survivors to speak openly about their experiences and is a crucial step towards preventing further FGM cases.
References:
-
Female genital mutilation. World Health Organization (https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation, accessed 19 July 2020)
-
Vacation Cutting: An Illegal Practice Still Running Rampant. AHA Foundation (https://www.theahafoundation.org/vacation-cutting-an-illegal-practice-still-running-rampant/, accessed 21 July 2020)
-
Types of female genital mutilation. World Health Organization (https://www.who.int/sexual-and-reproductive-health/types-of-female-genital-mutilation, accessed 19 July 2020)
-
Leye, E., Eekert, N. V., Shamu, S., Esho, T., & Barrett, H. (2019). Debating medicalization of Female Genital Mutilation/Cutting (FGM/C): Learning from (policy) experiences across countries. Reproductive Health, 16(1). doi:10.1186/s12978-019-0817-3
-
Brief on the medicalization of female genital mutilation. UNFPA; 2018 (https://www.unfpa.org/resources/brief-medicalization-female-genital-mutilation, accessed 19 July 2020)